Full text (PDF, 1,591KB)
Loock, C., Suleman, S., Lynam, J., Scott, L., Tyler, I. Linking in and linking across using a RICHER Model: Social pediatrics and inter professional practices at UBC. UBCMJ. 2016: 7.2 (7-9).
Christine Loocka,°, MD FRCPC; Shazeen Sulemanb, MD MSc; Judith Lynamc, PhD RN; Lorine Scottd, MN NP(F); Ingrid Tylere, MD CCFP MHSc MEd FRCPC;
Citation info: UBCMJ. 2016: 7.2 (7-9)
°Corresponding author: cloock@cw.bc.ca
a Associate Professor, Department of Pediatrics, Faculty of Medicine, University of British Columbia,Vancouver, BC
b Department of Pediatrics, University of Toronto,Toronto, ON
c Professor, School of Nursing, University of British Columbia,Vancouver, BC
d Adjunct Professor, School of Nursing, University of British Columbia,Vancouver, BC
e Assistant Professor, Dalla Lana School of Public Health, University of Toronto,Toronto, ON
Christine Loock MD, FRCPC, (shown here with her team) is a developmental pediatrician at Children’s and Women’s Health Centre of British Columbia, including Sunny Hill Health Centre for Children and BC Children’s Hospital where she is medical director of the Cleft Palate/ Craniofacial Program and specialist lead for the Social Pediatrics RICHER Program. A distinguished teacher and clinical researcher, she is an Associate Professor in the Department of Pediatrics, Faculty of Medicine, University of British Columbia (UBC). Early in her medical training at Harvard and the University of Washington, she developed an interest in ‘Social Pediatrics’. Her earlier clinical and research work focused on children and youth with congenital conditions and developmental disorders, including Fetal Alcohol Spectrum Disorders (FASD) and birth defects prevention. She has been a board member on the Canadian Centre on Substance Abuse and co-author of the Canadian National Guidelines for Diagnosis of Fetal Alcohol Spectrum Disorders. Over the past decade she has been engaged in collaborative interdisciplinary research to practice partnerships with [Lynam et al] UBC School of Nursing to develop innovative and effective ‘RICHER’ health service delivery models for socially vulnerable children and families in Canada. Dr. Loock is a recipient of the 2012 Queen’ Diamond Jubiilee Medal for community service awarded by the Governor General of Canada.
Back row left: Eva Moore, Judy Lynam, Chris Loock, Kristina Pikksalu, Lorine Scott, Clea Bland,Tamera Stilwell, Jane Hailey, Natasha ProdanBhalla, Gwyn McIntosh,Tram Nguyen. Front left: Shazeen Suleman, Denise Hanson, Joan McNeil, Curren Warf, Dzung Vo. Not pictured;Ashley Roberts, Mia Remington, Kelly Luu, Kelley Zwicker, Grace Yu, Myles Blank, Wingfield Rehmus,Warda Toma, Janet Greenman, Parveen Johal,Val Liao, Jaclyn Pennington,Vivian Nawrocki, Koushambhi Khan, Sabrina Wong, and Ingrid Tyler.
In 1991, the Canadian government vowed to eradicate child poverty by the year 2000. More than 20 years later, over 20% of children in Canada remain in poverty and conditions have deteriorated for children in the most vulnerable communities.1 British Columbia has the highest child poverty rate in Canada, with Vancouver’s Downtown Eastside (DTES) being one of Canada’s most at–risk and poorest neighbourhoods.2 There are no shortages of community organizations in the DTES—the Vancouver Sun reports over 260 agencies. Yet, the contributions of poverty and socio–economic conditions to health remain more significant than genetics or environment alone, as shown in Figure 1.3,4 Social and material poverty, and other adverse childhood experiences (ACEs) have been shown in many studies to be associated with poor neurodevelopmental and physical health outcomes.5,6 Living on the social margins not only limits children’s access to supports, it can also prompt them to question their social value and disrupt their sense of promise for a future.7 Moreover, population studies have shown that the impact of adversities are cumulative over the life course.8,9
However, early investments in children’s health and education have been shown to benefit children and society. Fostering connectedness and creating enduring social relationships have been shown to be protective against such forms of adversity as highlighted in Emmy Werner’s pioneering longitudinal study of Kauai’s children.10 Additionally, James Heckman, a Nobel prize laureate for economics, has shown that the estimated rate of return on investment for early childhood education is as high as 16%, which highlights the economic advantage of investing in vulnerable children.11
The RICHER model
Envisioned in 2006, the RICHER initiative (Responsive, Interdisciplinary, Intersectoral Child and Community Health Education and Research) developed as a collaborative partnership among interdisciplinary primary health care providers, including nurse practitioners, public health, family and specialist physicians, researchers, and community partners, to build evidence–based services for socially–isolated, marginalized, and materially– disenfranchised families in the DTES. RICHER serves an inner–city population of approximately 4000 children that includes new immigrants and Indigenous families, many of whom have experienced significant trauma, the effects of which can be profound for adults and children alike.
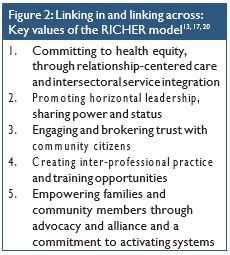
In the 2007-8 academic year, over two- thirds of children in the DTES neighbourhoods of focus were developmentally vulnerable at schoolentry,amongthehighestintheprovince.12 And while the current rates of vulnerability remain over 50%, with the implementation of RICHER and other community–driven,‘place– based’ strategies, there has been a ‘critical difference’ in vulnerability, with a decrease of almost 20%.12 RICHER’s interdisciplinary research–to–practice model has been recognized internationally for developing an effective health service delivery model that links into services and across sectors for socially vulnerable children and families.The key values and organizational features of RICHER, as outlined in Figure 2, are discussed below.13
Intersectoral service integration
Primary care providers and pediatric specialists provide direct health care to children and their families through scheduled consultations with individual families. At a community level, child development screening is performed in partner daycares. There is a kindergarten readiness screening program, initiated in 2014, which operates in partnership between the Vancouver School Board and Vancouver Coastal [Public] Health Authority. RICHER continues to grow along with a number of partnerships. It now offers access to a multitude of youth health services and dental services, and works to build the community infrastructure to create access to developmentally appropriate environments.
The needs of families and children drive the RICHER priorities. As a program of BC Children’s & Women’s Hospitals, RICHER partnerships have created access to public health, mental health, parent education and support programs, child care programs, legal services, and more. Most importantly, these services are distributed in neighbourhood spaces. Providers work in, and in partnerships with, schools, daycares, and community centres, including two evenings per week.
In 2015, RICHERmovedintoatownhouse in a public housing complex in the DTES.The townhouse was converted into examination rooms for children and youth, obstetrics and mental health, and includes a community kitchen and resource centre. With this move, RICHER has become a permanent part of the community fabric by being a literal “next– door neighbor” to families. RICHER members are invited to partner with local daycares, community centres, parent groups, and other community agencies to ensure culturally and developmentally appropriate supports for children, youth, and their families. By breaking down invisible barriers of power, culture, and location, and promoting care centered on relationships with families, children, and youth, the clinicians have effectively recognized and benefitted from the community’s expertise.13
Horizontal leadership
There is no one lead for the RICHER model as governance is horizontal.14 Every professional engaged in the RICHER initiative is accountable to their colleagues and to the families to foster responsiveness and respect, while maintaining high–quality services.RICHER values many different forms of expertise, as evidenced by the diversity of perspectives represented at their weekly community round– table discussions. Health care professionals and researchers learn from community members, who share their experience of living in poverty, and from elders, who provide insight into the social impact of residential schools. In the RICHER model, each voice is welcomed, acknowledged, and respected.
Engaging and brokering community trust
RICHER’s roots run deep and are embedded within pioneering partnerships with the Vancouver [Coastal] Health Department in research, policy, and primary health care service delivery. Early relationships forged with the community in the early 90’s with school and street nurses and not–for– profit agencies, such as YWCA Crabtree Corner, Vancouver Native Health, and
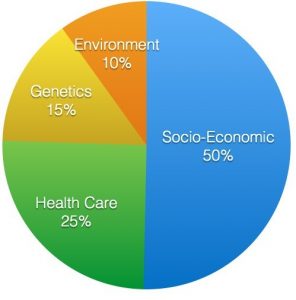
Figure 1: Determinants of health and their relative contributions to health.4
RayCam Community Cooperative, have led to the development of an innovative hospital community partnership with Children’s & Women’s Hospital and UBC. In these early years, the shared goal was to prevent adverse pregnancy outcomes (e.g. low birth weights, fetal alcohol syndrome, and neonatal abstinence syndrome) and the “separation of the mother–baby pair”.15 The Sheway Program (1993),YWCA Crabtree (1985) and Cause We Care Housing (opening 2016), and the “Our Place” Graduation strategy from the RayCam/NICCSS Networks are examples of interdisciplinary and intersectoral programs that have developed through community engagement and relationship building. By drawing on the expertise of several community champions, these connections have helped to broker trust.16 Prerequisites for successful engagement include nurturing longstanding relationships, spending time knowing, listening and understanding, and not parachuting into a community.17
Creating inter-professional practice and training
RICHER has also developed into an inter-professional clinical training site for public health, social work, medical, nursing, and law students. Rooted in service learning, students gain an understanding and appreciation for the impact of the social determinants of health on children, youth, and families. More importantly, they learn first–hand the benefit of working across sectors in partnership. UBC nursing and medical students and pediatric residents are sponsored to engage in weekly activities in the inner–city community daycares as part of their exposure to child development and advocacy. The MusicBox Children’s Charity of Canada is in its seventh year of sponsoring a community service learning option for second year medical students through required longitudinal courses emphasizing the bio–psychosocial model of care. This project combined MusicBox strategies to engage preschool–aged children who would otherwise have limited access to early music experiences with earlier developmental screening.
Empowering community through advocacy
Drawing on partnerships, RICHER has advocated within formal sectors to mobilize essential resources as needs have been identified. An overriding goal is to foster care that is responsive at the individual level and at the organizational level: a goal that is accomplished by ongoing dialogue with community partners and by working to ensure the perspectives of the community members are considered as plans are made. Key examples include work with Vancouver Coastal Health and BC Ministry of Education to screen for kindergarten readiness based on UBC’s Human Early Learning Partnership (HELP) data and to improve graduation rates for inner–city Aboriginal youth through the inner–city ‘Graduation Strategy’.12 These initiatives directly support several highly publicized provincial reports, reviews, and investigations of the BC Representative for Children and Youth,18 RICHER team members currently hold numerous leadership roles (e.g. Children and Youth with Special Needs, Circle of the Child and the Youth Matters Forum) to address improved services and case management for higher–risk children in care and youth in transition. They also partner with key community agencies, emergency room services, mental health and social work services (i.e. BC Ministry for Child and Family Development (MCFD) and Child and Youth Mental Health Services), and municipal police. Encouraging community initiated programs, such as NASKARZ [‘Never Again Steal Cars’], exemplify the effectiveness of respectful and enduring partnerships across sectors with target populations to enhance their social capital.19 Advocacy is about ‘working with’ and not just ‘working for.’
Research: measuring the impact of RICHER
We have knowledge of conditions that can mitigate the impact of social and material adversities and we have sought to harness these in the RICHER approach. The participatory approach used in our research enabled us to capture the key structural features and characteristics of RICHER’s clinical engagement.20 Our research has demonstrated that this model fosters access to quality primary health care for this vulnerable population.14 Our research has also demonstrated characteristics of the patient–provider relationship associated with an outcome measure of parental empowerment which is characterized by improved knowledge and the capacity to activate systems, as well as manage child and youth health conditions.13,14,20 Population research through UBC’s Human Early Learning Partnership (HELP) continues to capture significant improvements in child developmental vulnerability in DTES neighbourhoods. In other words, RICHER has been a good investment. By investing in children and youth, we have the opportunity to improve the health of the entire population.
“It is better to build strong children than repair broken men.” – Frederick Douglass
Disclosures
The authors do not have any conflicts of interest to disclose.
References
- Children of the recession: The impact of the economic crisis on child well–being in rich countries, Innocenti Report Card 12 [Internet]. Florence: UNICEF Office of Research; 2014 Sep [cited 2015 Nov 7]. Available from: http://www. unicef-irc.org/publications/pdf/rc12-eng-web.pdf
- First Call: BC Child and Youth Advocacy British Columbia 2014 Child Poverty Report Card [Internet].Vancouver: First Call: BC Child andYouth Advocacy Coalitition; 2014 Nov [cited 2015 Nov 7]. Available from: http://still1in5.ca/wp-content/ uploads/2014/11/First-Call-Coalition-Report-Card- 2014-FINAL-WEB.pdf
- Culbert L, McMartin Downtown Eastside: 260 agencies, housing sites crowd Downtown East- side. Vancouver Sun. [Internet]. 2014 Jun 27. [cited 2015 Nov 7]. Available from: http://www.vancou- versun.com/health/Downtown+Eastside+agen- cies+housing+sites+crowd+Downtown+East- side+with+video/9983274/story.html
- Marmot M, Allen Social Determinants of Health Equity. A J Public Health. 2014 Sep;104(S4):S517-9.
- Luby J, Belden A, Botteron K, Marrus N, Harms MP, Babb C, et The effects of poverty on child- hood brain development. JAMA Pediatr. 2013 Dec;167(12):1135 42.
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, EdwardsV, Koss MP, Marks Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) study. Am J Prev Med. 1998 May;14( 4): 245-58.
- Lynam MJ, Cowley Understanding marginaliza- tion as a social determinant of health. Crit Public Health. 2007 Jun;17(2):137 49.
- Power C, Hertzman C, Matthews S, Manor So- cial differences in health: Life-cycle effects between ages 23 & 33 in the 1958 British birth cohort. A J of Public Health. 1997 Sep;87(9):1499-503.
- Power C, Stansfeld S, Matthews S, Manor O, Hope
- Childhood and adulthood risk factors for so- cio-economic differentials in psychological distress: Evidence from the 1958 British birth cohort. Soc Sci & Med. 2002 Dec;55(11):1989-2004.
- Werner, , High risk children in young adulthood: A longitudinal study from birth to 32 years. Am J Orthopsychiatr. 1989 Jan;59(1):72-81.
- Heckman JJ, Masterov, The productivity argu- ment for investing in young children [IZA Discus- sion Paper No. 2725]. 2007 Apr. [cited 2015 Nov 7].Available from: http://ssrn.com/abstract=982117
- Human Early Learning [Internet].Van- couver, BC: University of British Columbia; 2014. [cited 2015 Nov 9].Available from: http://earlylearn- ing.ubc.ca/maps/edi/nh/critical-difference?sd=39
- Tyler I, Feller A, Ford-Jones L, Loock C, Lynam J, Makin S, et Social pediatrics realist review. Pre- sented at: The Ontario Public Health Conference (TOPHC); 2015 Mar 26;Toronto, CA.
- Lynam MJ, Scott L, Loock CL,Wong The RICHER social pediatrics model: Fostering access and reduc- ing inequities in children’s health. Healthc Q. 2011 Oct;14 Special Issue(3):41 56.
- Loock CA, Kinnis C, Robinson GC, Segal S, Blather- wick FJ, Armstrong Targeting high risk families: Prenatal alcohol/drug abuse and infant outcomes. Vancouver, B.C.: Department of Pediatrics, Faculty of Medicine, University of British Columbia;1993.
- Lynam MJ, Grant E, Staden Engaging with com- munities to foster health:The experience of inner– city children and families with learning circles. Can J Nurs Res. 2012 Jun;44(2):86 106.
- Wong ST, Lynam MJ, Khan KB, Scott L, Loock The social pediatrics initiative: A RICHER model of primary health care for at risk children and their families. BMC Pediatr. 2012 Oct;12:158.
- British Columbia’s Representative for Children and Paige’s story: abuse, indifference and a young life discarded [Internet]. Victoria: 2015 May [cited from 2015 Nov 9], 80 p. Available from: https:// www.rcybc.ca/sites/default/files/documents/pdf/re- ports_publications/rcy-pg-report-final.pdf
- NASKARZ Turning [Web streaming video]. 2014 Feb [cited 2015 Dec]. Available from: http:// byutv.org/watch/0256de75-38d7-4b47-9b54-eb- 46cd1ae881/turning-point-naskarz#ooid=RzaH- JrazoXPAWncP_tLJKWlQ5HM2NE1X
- Lynam MJ, Loock C, Scott L, Wong S, Munroe V, Palmer Social pediatrics: Creating organizational processes and practices to foster health care access for children ‘at risk’. J Res Nurs. 2010 Jul;15(4):331 47.